Desloratadine, pseudoephedrine sulphate.
The blue immediate release (IR) layer contains 2.5 mg of desloratadine and the white sustained release (SR) layer contains 120 mg of pseudoephedrine sulphate.
Excipients/Inactive Ingredients: hypromellose 2208, microcrystalline cellulose, povidone, magnesium stearate, silicon dioxide, corn starch, edetate sodium, citric acid, stearic acid, and Indigo Carmine E132 Aluminum Lake.
Pharmacology: Desloratadine is a long acting tricyclic histamine antagonist with selective H1-receptor histamine antagonist activity. Receptor binding data indicates that at a concentration of 2 - 3 ng/ml (7 nanomolar), desloratadine shows significant interaction with the human histamine H1 receptor. Desloratadine has an antihistamine potency approximately 3.5 - 20 times greater than loratadine in vitro and 2.5 - 4 times greater than loratadine in animals. Desloratadine inhibited histamine release from human mast cells in vitro. Results of a radiolabeled tissue distribution study in rats and a radioligand H1-receptor binding study in guinea pigs showed that desloratadine did not readily cross the blood brain barrier.
Pseudoephedrine sulphate is an orally active sympathomimetic amine and exerts a decongestant action on the nasal mucosa. Pseudoephedrine sulphate is recognized as an effective agent for the relief of nasal congestion due to allergic rhinitis. Pseudoephedrine produces peripheral effects similar to those of ephedrine and central effects similar to, but less intense than, amphetamines. It has the potential for excitatory side effects.
Pharmacodynamics: Wheal and Flare: Human histamine skin wheal studies following single and repeated 5 mg doses of desloratadine have shown that the drug exhibits an antihistaminic effect by 1 hour; this activity may persist for as long as 24 hours. There was no evidence of histamine-induced skin wheal tachyphylaxis within the desloratadine 5 mg group over the 28-day treatment period.
Effects on QTc: In clinical trials for AERIUS D-12 Tablets, ECGs were recorded at baseline and endpoint within 1 to 6 hours after the last dose. The majority of ECGs were normal at both baseline and endpoint. No clinically meaningful changes were observed following treatment with AERIUS D-12 Tablets for any ECG parameter, including the QTc interval.
Pharmacokinetics: Absorption and Bioavailability: In a single dose pharmacokinetic study, the mean time to maximum plasma concentrations (Tmax) for desloratadine occurred at approximately 4-5 hours post dose and mean peak plasma concentrations (Cmax) and area under the concentration-time curve (AUC) of approximately 1.09 ng/mL and 31.6 ng⋅hr/mL, respectively, were observed. In another pharmacokinetic study, food and grapefruit juice had no effect on the bioavailability (Cmax and AUC) of desloratadine. For pseudoephedrine, the mean Tmax occurred at 6-7 hours post dose and mean peak plasma concentrations (Cmax) and area under the concentration-time curve (AUC) of approximately 263 ng/mL and 4588 ng·hr/mL, respectively, were observed. Food had no effect on the bioavailability (Cmax and AUC) of desloratadine or pseudoephedrine.
Following oral administration of AERIUS D-12 Tablets dosed twice daily for 14 days in normal healthy volunteers, steady state conditions were reached on day 10 for desloratadine, 3-hydroxydesloratadine and pseudoephedrine. For desloratadine, mean steady state peak plasma concentrations (Cmax) and area under the concentration-time curve (AUC 0-12hrs) of approximately 1.7 ng/mL and 16 ng⋅hr/mL were observed, respectively. For pseudoephedrine, mean steady state peak plasma concentrations (Cmax) and AUC (0-12 hrs) of 459 ng/mL and 4658 ng⋅hr/mL were observed.
Distribution: Desloratadine and 3-hydroxydesloratadine are approximately 82% to 87% and 85% to 89%, bound to plasma proteins, respectively. Protein binding of desloratadine and 3-hydroxydesloratadine was unaltered in subjects with impaired renal function.
Metabolism: Desloratadine (a major metabolite of loratadine) is extensively metabolized to 3-hydroxydesloratadine, an active metabolite, which is subsequently glucuronidated. Analysis of plasma desloratadine and 3-hydroxydesloratadine concentrations showed similar Tmax and half-life values for both compounds.
The enzyme(s) responsible for the formation of 3-hydroxydesloratadine have not been identified.
Data from clinical trials with desloratadine indicate that a subset of the general population has a decreased ability to form 3-hydroxydesloratadine, and are poor metabolizers of desloratadine. In pharmacokinetic studies (n=3748), approximately 6% of subjects were poor metabolizers of desloratadine (defined as a subject with an AUC ratio of 3-hydroxydesloratadine to desloratadine less than 0.1, or a subject with a desloratadine half-life exceeding 50 hours). These pharmacokinetic studies included subjects between the ages of 2 and 70 years, including 977 subjects aged 2-5 years, 1575 subjects aged 6-11 years, and 1196 subjects aged 12-70 years. There was no difference in the prevalence of poor metabolizers across age groups. The frequency of poor metabolizers was higher in Blacks (17%, n=988) as compared to Caucasians (2%, n=1462) and Hispanics (2%, n=1063). The median exposure (AUC) to desloratadine in the poor metabolizers was approximately 6-fold greater than in the subjects who are not poor metabolizers. Subjects who are poor metabolizers of desloratadine cannot be prospectively identified and will be exposed to higher levels of desloratadine following dosing with the recommended dose of desloratadine. In these studies, no overall differences in safety were observed between poor metabolizers and normal metabolizers.
Pseudoephedrine alone, is incompletely metabolized in the liver by N-demethylation to an inactive metabolite. The drug and its metabolite are excreted in the urine. About 55-96% of an administered dose of pseudoephedrine hydrochloride is excreted unchanged in the urine.
Elimination: Following single dose administration of AERIUS D-12 Tablets, the mean plasma elimination half-life of desloratadine was approximately 24 hours.
When administered alone, the mean elimination half-life of pseudoephedrine is approximately 4-6 hours which is dependent on urine pH. The elimination half-life is decreased at urine pH lower than 6 and may be increased at urine pH higher than 8.
AERIUS D-12 Tablets are indicated for the relief of the nasal and non-nasal symptoms of allergic rhinitis, including nasal congestion, in adults and children 12 years of age and older.
Aerius D-12 Tablets should be administered when the antihistaminic properties of desloratadine and the nasal decongestant activity of pseudoephedrine are desired.
Adults and adolescents (≥ 12 years of age): One AERIUS D-12 Tablet twice a day regardless of mealtime. For oral use.
Caution: Do not chew, break or crush the tablet. Swallow whole.
The duration of treatment should be kept as short as possible and should not be continued after the symptoms have disappeared. The incremental efficacy of pseudoephedrine over desloratadine alone has not been studied beyond a duration of two weeks.
In the event of overdose, consider standard measures to remove any unabsorbed drug. Symptomatic and supportive treatment is recommended.
Desloratadine and 3-hydroxydesloratadine are not eliminated by hemodialysis.
AERIUS D-12 Tablets are contraindicated in patients who are hypersensitive to the active substance, to any of its excipients, to adrenergic agents or to loratadine.
As Aerius D-12 contains pseudoephedrine, it is also contraindicated in patients who are receiving monoamine oxidase (MAO) inhibitor therapy or within fourteen (14) days of stopping such treatment.
Aerius D-12 is also contraindicated in patients with: narrow-angle glaucoma, urinary retention, severe hypertension, severe coronary artery disease, hyperthyroidism, a history of haemorrhagic stroke or with risk factors which could increase the risk of haemorrhagic stroke. This is due to the alpha-mimetic activity of pseudoephedrine in combination with other vascoconstrictors such as bromocriptine, pergolide, lisuride, cabergoline, ergotamine, dihydroergotamine or any other decongestant medicinal product used as a nasal decongestant, either by oral route or by nasal route (phenylpropanolamine, phenylephrine, ephedrine, oxymetazoline, naphazoline…).
AERIUS D-12 Tablets should be used with caution in patients with hypertension, diabetes mellitus, ischemic heart disease, increased intraocular pressure, hyperthyroidism, renal impairment, liver impairment or prostatic hypertrophy. Central nervous system stimulation with convulsions or cardiovascular collapse with accompanying hypotension may be produced by sympathomimetic amines.
Severe skin reactions such as acute generalized exanthematous pustulosis (AGEP) may occur with pseudoephedrine-containing products. Patients should be carefully monitored. If signs and symptoms such as pyrexia, erythema, or many small pustules are observed, administration of this drug should be discontinued and appropriate measures taken if needed.
Desloratadine should be administered with caution in patients with a medical or family history of seizures. In particular, young children may be more susceptible to developing new seizures under desloratadine treatment. Healthcare providers may consider discontinuing desloratadine in patients who experience a seizure while on treatment.
Use in Children: AERIUS D-12 Tablets are not appropriate dosage forms in pediatric patients and are not recommended in patients under 12 years of age due to a lack of data on safety and efficacy.
Use in Elderly: Elderly patients are more likely to have adverse reactions to sympathomimetic amines. Dose selection for elderly patients should be cautious, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy in this population.
There have been no reproduction studies conducted with the combination of desloratadine and pseudoephedrine. There are no adequate and well-controlled studies in pregnant women. Desloratadine has not been shown to be teratogenic in animal studies. However, because animal reproduction studies are not always predictive of human response, desloratadine should be used during pregnancy only if clearly needed.
Desloratadine and pseudoephedrine both pass into breast milk. Therefore a decision should be made whether to discontinue nursing or to discontinue AERIUS D-12 Tablets taking into account the importance of the drug to the mother. Caution should be exercised when AERIUS D-12 Tablets are administered to a nursing woman.
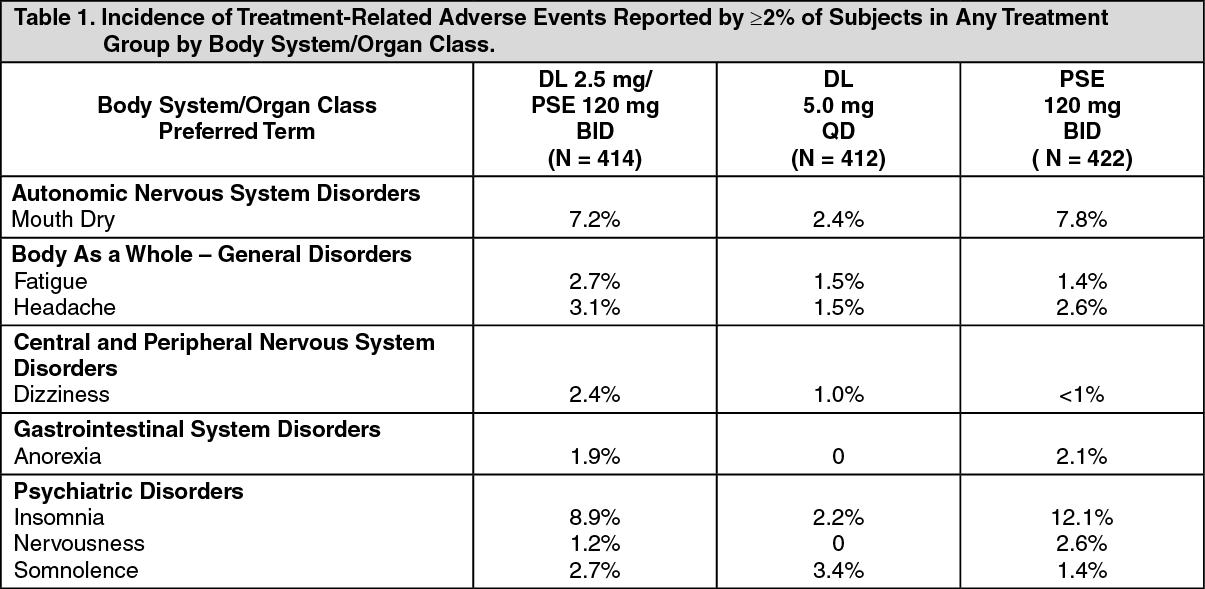
The safety of AERIUS D-12 Tablets was studied in 414 patients who received AERIUS D-12 Tablets twice daily for up to two weeks. The majority of adverse events that occurred following treatment with AERIUS D-12 Tablets were similar in type and frequency to those observed in patients treated with pseudoephedrine alone. Treatment related adverse events reported by ≥ 2% of patients are listed in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The following spontaneous adverse events have been reported during the marketing of desloratadine as a single ingredient product: hypersensitivity reactions (including anaphylaxis and rash), tachycardia, palpitations, psychomotor hyperactivity, seizures and elevated liver enzymes (including bilirubin and hepatitis), and increased appetite have been reported very rarely.
Cases of severe skin reactions such as acute generalized exanthematous pustulosis (AGEP) have been reported with pseudoephedrine-containing products.
No specific interaction studies have been conducted with AERIUS D-12 Tablets. However, in clinical pharmacology studies in healthy volunteers, there were no clinically relevant changes in the safety profile of desloratadine when co-administered with erythromycin, ketoconazole, azithromycin, fluoxetine and cimetidine as assessed by electrocardiographic parameters (including the corrected QT interval), clinical laboratory tests, vital signs and adverse events (see Table 2).
Click on icon to see table/diagram/image
The antihypertensive effects of beta-adrenergic blocking agents, methyldopa, mecamylamine, reserpine, and veratrum alkaloids may be reduced by sympathomimetics.
Increased ectopic pacemaker activity can occur when pseudoephedrine is used concomitantly with digitalis.
Store below 30ºC. Store in original package. Protect from excessive moisture.
R01BA52 - pseudoephedrine, combinations ; Belongs to the class of systemic sympathomimetic preparations used as nasal decongestants.
Aerius D-12 MR tab
10 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image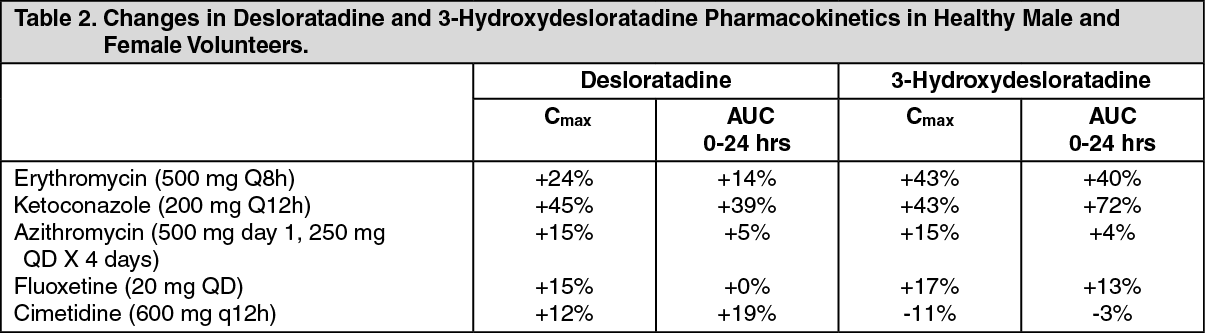 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
